
Patient is a 67 year old female with a history of pharmacologically controlled hypertension and hypothyroidism.
Tooth #14 was removed approximately 6 months previously due to the presence of pain and a firm buccal alveolar swelling of 2 month duration. Due to the anatomic position of the zygomatic process in this patient, plain radiography was of minimal diagnostic value. Cone beam CT confirmed periradicular pathology. Root fracture was suspected preoperatively and was confirmed the day of tooth removal.
The large defect was grafted with mineralized particulate allograft using a guided bone regeneration technique.
The large defect was grafted with mineralized particulate allograft using a guided bone regeneration technique.
Patient was treatment planned for a dental implant at site #14 with a closed sinus lift after a 6 month healing period.
Tooth #13 is treatment planned for a new restoration.
__________________________________________________________
__________________________________________________________

Preoperative coronal cone beam image of tooth #14 demonstrating a large well contained periapical lesion along the floor of the maxillary sinus.

6 month postoperative periapical radiograph illustrating the appearance of the grafted area.


At surgery, bone was noted to be dense (D1).

Final sinus lift osteotome used to depth (~13mm).

4.7mm x 11.5mm Zimmer Trabecular Metal Implant.

Implant insertion torque value was greater than 35 Ncm.
Osstell reading was taken to determine implant stability.

Osstell ISQ implant stability value was 75 at insertion.
(For reference, implants that are ready for final restoration will typically have an ISQ value of 65 or greater.)

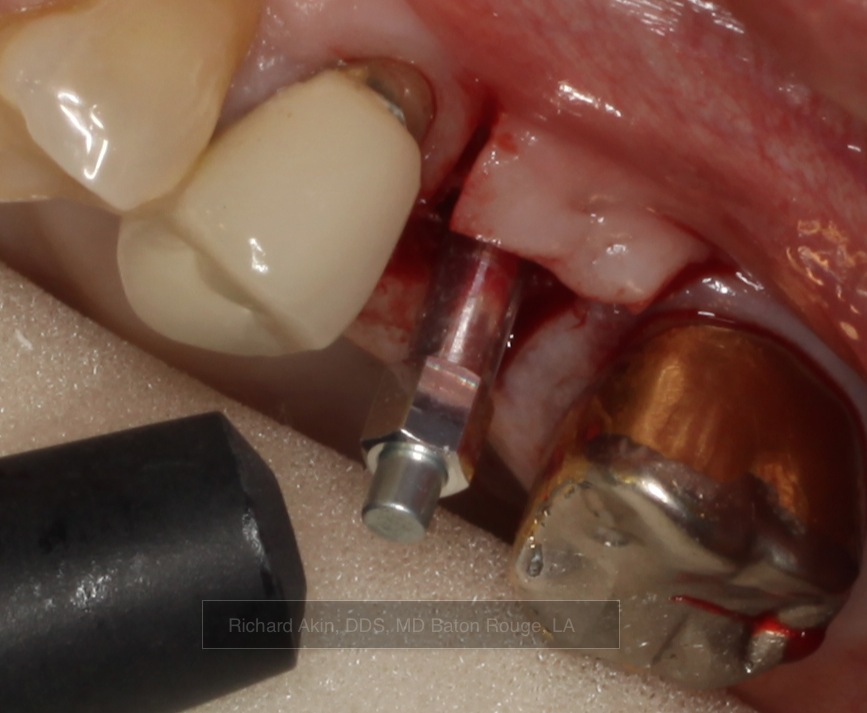
Implant at final depth.

Palatal tissue was contoured to accept healing abutment using a rotary tissue punch.

The highlight of my trip to Parsippany, NJ! I thoroughly enjoyed it.
concept sounds great, among other things, increasing area of attachment...does this imply shorter and narrower implants? the one pictured does not look smaller
ReplyDeleteIt is a must for you to call me to watch you take the first one out that fails! If one ever does. For instance, bonehead gp like me, getting excess cement on the implant threads! ;)
ReplyDeleteSteve, I think that current implementation is conservative (as it should be.) The implant is the identical diameter of the TSV implant although it may prove to be a great surface for small diameter implants, possibly with less dense bone applications or even as a crystal option.
ReplyDeleteAs Dustin said, it will be interesting to see how the bone behaves within the trabecular metal when subjected to an inflammatory stimulus (ie. peri-implant inflammation.)
I would expect that removal would not be too difficult especially with Piezosurgery and thin tapered fissure burs. These techniques cause very little collateral bony damage. Trephine burs should no longer be used to remove implants - these 'maximally invasive' techniques should be a thing of the past.
That should be 'crestal' options, not crystal.
ReplyDeleteI´m hungry for papers about this trabecular metal implants, mainly clinical trials. If you have some, please send me the references. Thank you and congratulations for the nice job.
ReplyDelete